


How Much Alcohol Should You Drink? Part 2


This Halloween it's hard to imagine anything scarier than the 2024 presidential election.
If anxiety about the wrong candidate winning (or falsely claiming a win) is driving you to drink, you've come to the right place. I'll be discussing two questions here:
1. How much alcohol can one drink without increasing the risk of health problems?
2. Is there a level of alcohol consumption that benefits health without increasing the risk of health problems?
According to some authorities, the answer to the first question is: None. For instance, since 2023, the World Health Organization's official position has been that there's no safe level of alcohol consumption. Is that a fair statement?
I will suggest that light drinking doesn't increase health risks, or at least not enough for most people to have cause for concern. That's my reading of the data. But I won't pretend that it's easy to define "light drinking".
The second question asks whether there's a sweet spot: Is there some degree of "light drinking" that actually benefits health without increasing the risk of harm? I will suggest that some individuals have a sweet spot, but recent evidence doesn't show that most of us would.
As I noted last week, the perils of drinking have been noted for thousands of years, but only during the past century have statistical methods and computing power advanced to the point that we can distinguish between the effects of slight differences in amount of consumption. In a word, we have great tools.
Observational data
How are those tools leveraged? How do scientists explore the health risks of drinking alcohol?
The most common approach is the observational study, where people describe their own drinking behavior, and information about their health is recorded.
The most recent large-scale observational study was published this August in JAMA Network Open. The researchers, led by Rosario Ortolá at Autonomous University of Madrid, looked at mortality rates among 135,103 older drinkers over a period of two to 15 years.
Ortolá and colleagues classified participants into four groups according to how much alcohol they reported drinking. The unit of measurement was grams (g).
In the U.S., one standard drink is defined as containing 14 grams of alcohol. That's roughly equivalent to one 12-ounce beer, one 5-ounce glass of wine, or one 1.5-ounce shot.
The table below shows how Ortolá and colleagues defined their four groups.

You can see, for example, that averaging one drink per day (14 grams) would lead a man to be classified as low-risk and a woman to be classified as moderate-risk.
(Values differ for men and women because women tend to be smaller and have a higher percentage of body fat, less body water, and less of an enzyme released by the liver that metabolizes alcohol.)
In their main analyses, Ortolá and colleagues compared the three alcohol risk groups to the occasional drinkers. Here are the two main findings:
—Among healthy individuals who live in relatively affluent areas, higher mortality rates were only observed among the high-risk group.
—Among individuals with health risks who live in relatively poor areas, higher mortality rates were found for each alcohol risk group. (Specifically, higher cancer mortality rates for all three groups, higher all-cause mortality for the moderate-risk and high-risk groups, and higher cardiovascular disease mortality for the high-risk group).)
Concretely speaking, here's what the results imply:
—If you're fairly healthy and not poor, you can be a light drinker without reducing your life expectancy. The upper limit is about 20 to 40 grams per day for men (a drink-and-a-half to just under three drinks) and about 10 to 20 grams per day for women (about three-quarters of a drink to nearly a drink-and-half).
—If you have health issues and you're poor, you risk cutting years from your life if you drink more than about a fifth of a drink per day on average. That's slightly less than one drink per week.
A sober assessment
Ortolá et al.s' study was well-designed but limited by the way alcohol consumption was measured. It's worth describing the limitations, because they're reflected in all observational studies on this topic and influence any practical advice we might glean.
How did Ortolá and colleagues know how much their participants drank?
The researchers used data from the UK Biobank, an ongoing biomedical study of over half a million older adults (ages 40 to 69) who agreed to participate from 2006 until at least 2036.
At some point between 2006 and 2010, each participant completed an online survey in which they described their drinking behavior. Current drinkers estimated their average weekly and monthly consumption of different types of drinks (the screenshot below was provided by the UK Biobank; this isn't my personal data. As per UK standards, one unit equals about 8 grams.)

A number of big-data alcohol studies rely on the UK Biobank. Whether they do or don't, all self-report surveys of drinking behavior yield imprecise data. Why is that?
(a) People don't routinely measure how much they drink.
(b) Within each category (e.g., beer), products differ in alcohol content, and drinkers may or may not finish their drink on some occasions.
(c) People may forget, or misrepresent their alcohol consumption.
Some researchers argue that these issues result in underestimates of actual consumption. I don't see persuasive evidence for this. In my view the data are simply messy, and we can only hope that the errors somehow balance out.
Even if surveys managed to capture exactly how much participants drink, the data would be limited in other ways.
(d) Samples may not be representative.
Only about 5.5% of people invited to participate in the UK Biobank study actually joined. When asked about their drinking behavior, some participants chose a "prefer not to say" option. In short, the best-case scenario is precise measurements for a tiny segment of the population.
(e) Drinking behavior is measured once, or on a small number of occasions.
UK Biobank participants described their drinking behavior when they first joined the study between 2006 and 2010. Based on that single response, they were classified into one of the four groups, but the extent of their drinking may have changed over time. In short, the best-case scenario is a clear snapshot of their drinking behavior at one point in time.
(f) Participants describe how much they drink, on average, each week or month (as in the UK Biobank study) or on a "typical" day, week, or month.
Estimates like these don't capture different patterns of drinking. A person who drinks one beer every evening of the week has the same average consumption as a person who abstains all week and then drinks seven beers on Saturday night. Studies on binge drinking suggest poorer health outcomes for the second person. For instance, a study published last month showed that individuals who report binge drinking (at least 4 to 5 drinks in a single episode) on rare occasions (as little as once per month to once per year) increase their risk of hypertension.
My point is not that observational data is invalid but that it's messy. I don't think any of the studies call for measuring how much you drink down to the gram.
All the same, the literature does offer a useful message about light drinking.
I've combed through recent reviews of observational research on the relationship between drinking and cardiovascular disease, cancer and all-cause mortality. In most of these studies, you can find a low level of alcohol consumption that's not associated with elevated health risks. In other words, light drinking, up to a point, doesn't increase the risk of heart disease, cancer, or reduced life expectancy.
What does "up to a point" mean? The hard truth is that we can't trust overly specific limits (e.g., exactly 15 grams of alcohol per day):
—Researchers study ranges of consumption (e.g., 10 to 20 grams per day) rather than specific quantities.
—"Safe" levels of alcohol consumption vary from study to study.
—As I've noted, the data from any particular study will be imprecise.
—Researchers measure group risk. This provides general guidance that doesn't necessarily predict outcomes for individuals.

In the Dietary Guidelines for Americans, the USDA and HHS recommend two drinks or less per day for men, and one drink a day or less for women. (Again, a "drink" is roughly one 12-ounce beer, one 5-ounce glass of wine, or one 1.5-ounce shot.)
These guidelines seem roughly consistent with much of the observational data. Although most studies don't use these exact units of measurement, average daily consumption at something approximating these levels is rarely linked to increased health risks.
What about the bad news?
A few observational studies do show increased risk associated with the lowest levels of consumption measured. But this isn't as bad as it sounds, because the data are ambiguous.
For instance, why does the WHO now claim there's no safe level of alcohol consumption? In part because of evidence that light to moderate consumption increases the risk of cancer. But when you look at the actual data, "light to moderate" turns out to be defined as 0 to 20 grams per day.
Practically speaking, that's a wide range. It includes people who drink once or twice per year, people who take one drink per week, and people who take just a sip less than a drink-and-a-half per day, every day. I appreciate the WHO's cautiousness, but data like this doesn't rule out the possibility that light drinking incurs no risks.
I want to emphasize this point. When researchers draw conclusions like "no safe dose of alcohol for the brain was found" and journalists the reiterate the claim, readers may not realize that the researchers haven't actually demonstrated low-consumption effects.
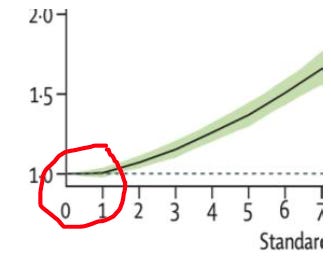
In some cases, we may be seeing bias rather than caution. In a 2018 Lancet study, for instance, researchers concluded that "the safest level of drinking is none." That's not what their data shows. Below is a screenshot from their Results section where they discuss data aggregated across a variety of health risks. In the text, they note that zero drinks per day minimizes risk, and that risk rises with any increase above zero consumption. They also refer the reader to Figure 5. Ok, let's look at the figure. It happens to be right next to the text. You can plainly see no difference in risk from zero to one drink per day. (The second screenshot below zooms in on the key area.) Bias seems to have influenced how the researchers viewed their own data!
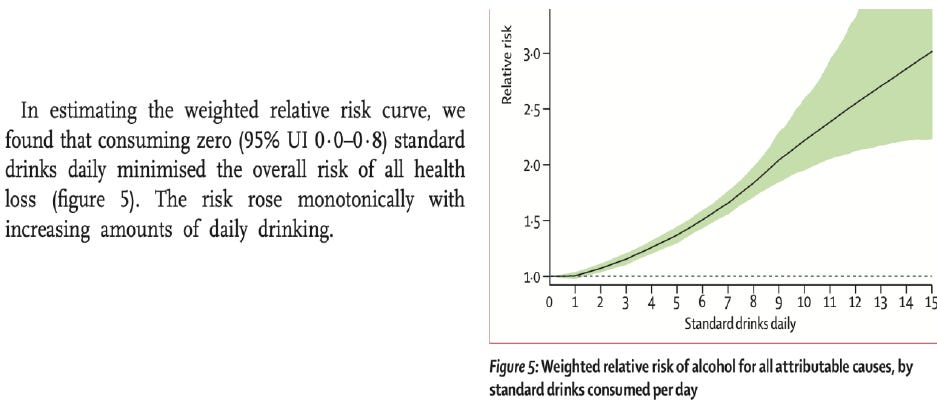
Finally, it's important to note that slightly exceeding"safe" thresholds identified in observational studies may not increase risk by much. The figure above, for instance, shows that the health risks of two drinks per day are roughly 5% greater than for one drink per day. Studies routinely show greater reductions in health risks for lifestyle variables such as more exercise or a healthier diet.
Please don't misunderstand that last comment. I'm not encouraging anyone to think: I can drink more so long as I also start jogging or cutting down on Big Macs. My point is simply that if we assume a safety threshold for alcohol consumption, exceeding that value by a small margin only slightly increases health risks.
I want to briefly discuss two alternatives to observational methods, then close with some hopefully useful takeaways.
RCT data
Observational data is inherent messy. Traditionally, the remedy is a randomized controlled trial, or RCT.
In an RCT, people are randomly assigned to conditions, a technical term simply meaning that they're asked to do something.
For instance, one group of people might asked to abstain from alcohol for six weeks. Another group would be asked to drink exactly one glass of wine per day during this time period. Yet another group would be asked to drink two glasses. Cardiovascular health might be measured at weeks 0 and 6.
Unfortunately, RCT data on the health effects of alcohol consumption is limited in scope.
One reason is impracticality. It would be hard to get people to agree to (and stick with) a certain drinking routine and then monitor their health for a period of years. There are also ethical concerns. Because alcohol is both dangerous and addictive, researchers typically can't ask people to drink much for very long.
I've looked at RCT meta-analyses published in 2011, 2020, and 2022. The studies included in these meta-analyses measured the health impacts of alcohol consumption anywhere from six hours after a single drink to about six months after consuming a specified amount each day. Control groups were typically asked not to drink. Outcomes included biochemical variables like cholesterol, measures of cardiovascular health such as blood pressure and arterial stiffness, and so on.
The data are inconsistent as to whether the lowest levels of drinking are beneficial, but I can at least say this: In the majority of RCT studies, light drinkers don't end up worse off than people who abstain. ("Light drinking" tends to be less than about a drink or two per day, depending on study.)
I don't think these studies tell us there's no safe level of alcohol consumption. Rather, as with observational research, the RCT data tends to show that beyond some point, the more people drink, the greater the risk of health problems. Like anything else, alcohol is toxic if you consume enough of it, but low levels of consumption may not be harmful.
MR data
A recently developed alternative to observational methods and RCTs is the Mendelian randomization study.
MR studies are grounded in evidence that genetic variants predict how much people will drink. Remember that model of DNA you studied in high school science? The one that looked like a twisted ladder? You may recall that the "rungs" of the ladder are made out of billions of nucleotide pairs.
For the most part, the sequence of pairs is the same from one person to the next. But out of those billions of "rungs", we each have a few million rungs where one of the nucleotides differs from the usual sequence. These are called "single nucleotide polymorphisms", or SNPs, and they contribute to physiological differences between people, including how we react to alcohol and thus how much we drink.

In MR studies, over 90 SNPs may be used to represent how much alcohol people actually consume, because there's evidence that these variables are associated. (If you're a stats person, you've probably guessed that MR studies reflect an instrumental variable approach.)
Broadly, the findings of MR studies are similar to those of recent observational studies and RCTs, except that some MR research suggests more strongly that even the lowest levels of alcohol consumption are harmful.
Another sober assessment
Now it seems like we should be worried.
MR studies avoid the messiness of observational data, because researchers aren't asking people to recall how much they drink. Rather, they're doing something more objective: Taking blood and identifying genetic variants.
MR studies also avoid the impracticality of RCTs, because the blood test can be done just once, and we can then monitor health outcomes over a period of years.
For these reasons, some researchers consider MR findings to be inherently stronger than observational evidence or even RCT studies on the topic.
All the same, there are good reasons to take MR data with a grain of salt (such as the kind one might find on the rim of a margarita glass).
One reason is that both alcohol consumption and health problems like cardiovascular disease may be driven by some other genetic contributor. If that's the case, then drinking would not be the primary cause of CVD. MR studies can't readily rule out this possibility.
The other issue stems from the indirectness of the MR approach. Is the exact amount of alcohol you drink determined by your genes? Of course not. Rather, a relationship between SNPs and alcohol consumed only emerges among large groups of people. The associations are moderate at best and suggest that quite a bit of variation in how much people drink can't be explained by their genes. Meanwhile, because the relationship between SNPs and alcohol consumption can only be established by asking people about their drinking behavior, we find ourselves once again contending with the messiness of self-reported measures of drinking.
I'm not saying that MR studies are invalid or uninformative. My point is that we shouldn't trust highly specific predictions from MR data any more than we should trust those arising from observational studies. MR studies simply confirm that alcohol is dangerous, and beyond a certain point, the more you drink, the greater the risks. I don't see good evidence for the claim that the lowest levels of drinking are harmful.
Conclusions
Here are four takeaways from this newsletter.
1. Guidelines for alcohol consumption are necessarily crude.
It's understandable that authorities ranging from international health organizations to your primary care physician recommend specific limits on how much to drink, but their advice tends to be more specific than the data can justify.
2. The more you currently drink, the more you'd benefit from a slight reduction.
Heavy drinking has been linked to cardiovascular disease, cancer, dementia, and a long list of more specific health problems. In many studies, the effects tend to be more exponential than linear, meaning that the more one currently drinks, the greater the impact of a slight increase in consumption.
This can also be expressed positively: The more one currently drinks, the greater the benefits of cutting back slightly.
Thus, in the figure below, it's the orange line rather than the blue one that captures the general relationship between alcohol and health risks.

Starting from the far left side of the figure and moving rightward, the orange line shows that drinking a little more doesn't increase risk much. The further right you move, the more sharply the line trends upward. The practical implications are clear:
—If you're a light drinker, a small change in how much you drink won't have much impact on health risks.
—If you drink a lot, a small change in how much you drink will have more impact on the health risks. Scaling back could have meaningful benefits.
3. Light drinking might not appreciably increase the risk of health problems.
At what level of consumption does that orange line start to curve upward?
The two major health organizations in the U.S. that provide recommendations use different language to express similar answers to this question.
—The CDC defines "excessive" drinking as a weekly average of eight or more drinks for women (i.e., just over one drink per day), and 15 or more drinks for men (i.e., just over two drinks per day). The CDC notes that lower levels may still be risky, but the agency is vague as to whether there may be a safe level of consumption.
—In the Dietary Guidelines, the FDA and HHS recommend similar but fractionally more conservative limits: one drink or less per day for women, two drinks or less per day for men. These are not meant to be averages but daily limits. Here too, it's left ambiguous whether a lower level of consumption might be safe.
Canada's Guidance on Alcohol and Health is noticeably more conservative. Three to six drinks per week (i.e., less than one per day) is said to increase the risk of cancer, while one to two drinks per week is described as "likely to avoid health consequences".
The WHO, as I've mentioned, is most conservative of all, because the organization claims there's no safe level of consumption. The risk to drinkers' health "starts from the first drop of any alcoholic beverage," according to their 2023 press release.
It's understandable that health organizations would be cautious and that, if anything, they err on the side of caution. The WHO does seem overcautious. The CDC and FDA/HHS recommendations seem more aligned with what the most credible recent data shows, though they may be slightly too careful in their advice.
In the end, what we can glean from the data are estimates of group-level risk. Whether or not you are personally affected by light to moderate drinking depends on your particular genes, your lifestyle, and so on.
4. Light drinking might improve your health in some respects without increasing the risk of health problems.
Last week, I noted that although health benefits of light drinking have been documented, newer and more rigorously-designed studies have found no differences between, say, lifelong abstainers and light drinkers. Again, this is group data and individual outcomes vary widely. Some individuals, if they're not taking medicines or have health conditions (including a history of alcohol use disorder) that preclude alcohol consumption, may benefit from light drinking without increased risk of harm.
Can you know for sure whether you're one of those individuals? Probably not. Perhaps the best you can do is to ask yourself: Do I feel good during and after drinking? Do others express concerns about my drinking? Do I avoid using alcohol as a crutch for dealing with my problems? Do I avoid excessive consumption in the form of binge drinking or daily overindulgence? Am I sleeping well? If the answers to all of these questions are "yes", then perhaps you are indeed benefitting without risks to body or brain.
Thanks for reading!
Thank you! I realize there is no such thing as absolutely no risk to anything potentially bad for us! So, I feel much better checking off most of the healthy boxes here! Thanks again Dr Springer. You made my day!
Hi Dr Springer - Thank you for your great reporting! My question is, do these studies take into consideration smoking , obesity and HPV in their case studies (participants) to alcohol causing specific cancers? Smoking/tobacco alone can cause up to 89 % of many of the 7 cancers. There are 7 cancers that are caused by alcohol as per reported by Surgeon General Murthy in 2025. I am wondering if overall habits, lifestyle or infections are recorded when making their assessments of cancer risk from alcohol?