

Is Drug Decriminalization Working?

I've been thinking about this newsletter for almost a year now.
One morning last November, returning home from the playground with my granddaughter, I noticed a young couple sitting on the landing outside my apartment building. The woman was pressing a syringe into the man's arm.
In a sense, there was nothing unusual about this scene. We lived in Cambridge Massachusetts, right around the corner from a Central Square intersection where drugs are often sold and openly used.
My initial reaction was pretty typical too. I didn't think about opioid statistics or Cambridge's 2021 decriminalization law. I didn't feel sympathetic toward the couple. I just wanted them to stay the hell away from my granddaughter. Go shoot up somewhere else, I thought. NIMBY.
Then, for some reason, I was struck by the absurdity of the situation. There we were, citizens of the richest country in the world, living among some of the smartest people in the world (Harvard and MIT are each less than a mile away), yet this disheveled couple still ended up on my landing, sharing a needle. Why couldn't we prevent this from happening?
Time passed, I tried (often unsuccessfully) to be more sympathetic toward the Central Square users, and then, last week, I came across a new study on the impact of drug decriminalization. The study is informative. It illustrates the power of statistics to address important social problems. It illustrates some of the limits on what statistics can tell us. And, in conjunction with the stories people are telling, it hints at the kinds of solutions that will and won't be effective.
The problem
In 1971, President Nixon declared a "war on drugs", and new era of drug policy was born: Stricter laws, greater enforcement, more incarceration.
Exactly 50 years later, responding to an ACLU poll, 83% of Americans said that we've lost the war on drugs. Most experts agree. Since the 1990s we've been experiencing an opioid epidemic that grows worse each year owing to the emergence of new opioids (fentanyl), modified opiods ("tranq", or fentanyl plus xylazine), and even "classic" opioids resurfacing in new recipes ("purple drank", aka "lean" – cough syrup containing codeine and the sedative promethazine, mixed with soda).
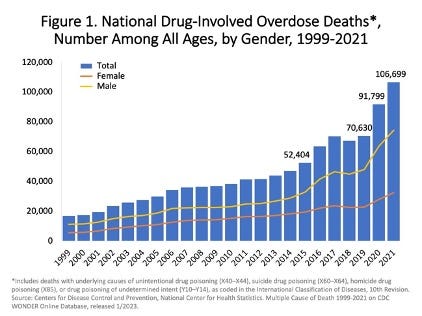
The opioid epidemic is more accurately called a "drug epidemic", because other highly addictive, lethal drugs such as methamphetamine are increasingly undermining public health, crime, and local economies. The figure below, drawn from CDC data, focuses on just one variable – overdose fatalities – but the upward trend conveys the broader theme.
The decriminalization debate
Decriminalization – a reduction in the legal penalties for drug possession and other drug-related activity – is an alternative to the war on drugs that has become increasingly popular. (My focus here is on the most dangerous drugs rather than say, possession of small quantities of marijuana.)
Supporters of decriminalization view drug abuse as a health issue rather than a criminal one. They argue that prevention and treatment are more effective than punishment, because users will be more willing to seek help, and more help will be provided. Other benefits include lower costs, less racial disparity in drug-related incarceration, and lower rates of HIV infection.
Opponents of decriminalization argue that reducing penalties for drug use simply encourages more drug use. By reducing the consequences, while sending the message that it's only a minor transgression, drug use will increase in both prevalence and openness. In other words, there won't just be more users, but more users out on the street, endangering or at least annoying the general public.
Which position makes more sense? Do we send the couple on my landing to a social worker or put them in jail? Until recently, we had no data on the decriminalization of the most dangerous drugs, because no state substantially decriminalized them. Two years ago, that began to change.
The decriminalization "experiments"
In February 2021, new drug decriminalization laws went into effect in Oregon and Washington. The new laws create natural experiments, allowing us to explore how drug-related outcomes in each state changed after the laws took effect.
What's special about these decriminalization "experiments" is that they apply to all illegal drugs, including the most dangerous ones.
In Oregon, Ballot Measure 110 reclassified the possession of small amounts of previously criminalized drugs as a noncriminal violation. The offender receives a fine of $100, which is waived if they seek a health assessment within 45 days (with further support offered during the assessment).
In Washington, a Supreme Court decision and a new bill, SB 5476, reduced most drug possession crimes to misdemeanors. Arrests could not be made for low-level drug offenses unless the person had been referred for assessment and treatment at least twice, and law enforcement officers could continue to offer referrals indefinitely instead of making an arrest. (I'm using the past tense here, because in July 2023, Washington toughened these laws, though not to pre-2021 levels.)
So, what was the impact of the new laws on the drug crisis, particularly for the most lethal drugs?
When you evaluate the effects of a new policy, you can listen to the stories or you can look at the statistics. Stories and statistics may agree, disagree, or, as in the case of Oregon and Washington, inform us about different things. I'll start with the statistics – the only ones available to date in peer-reviewed research.
The new study
Two weeks ago, JAMA Psychiatry published a study led by Dr. Spruha Joshi at the NYU School of Medicine that focused on one outcome: overdose deaths in Washington and Oregon following decriminalization. CDC death certificate data was used to identify a pre-decriminalization time period (January 1, 2018 throuh January 31, 2021) as well as a one-year period following the February 2021 decriminalization in each state.
(Although type of drug wasn't distinguished, the use of mortality data meant that the study focused in effect on fentanyl and methamphetamine overdoses. According to CDC data, during the past two years fentanyl was responsible for over 70% of fatal overdoses, while another 25% or so can be attributed to methamphetamine.)
Broadly speaking, data from these states could be analyzed in two ways:
1. Before vs. after comparisons.
The obvious thing to do is to compare overdose rates before and after the new laws took effect. If overdoses increase, for instance, we would conclude that decriminalization made the drug problem worse.
This approach is not ideal, in part because overdose rates in all states, including these two, have been increasing dramatically in recent years. A continued increase after the new laws kick in doesn't prove that the laws were ineffective. For all we know, overdose rates would've been even worse without the laws. This is one reason Joshi and colleagues used a different analytic approach.
2. Control group comparisons.
If you're a fan of science fiction, a theoretical physicist, or a philosopher, you might say: The obvious thing to do is to compare overdoses in Oregon following the new laws to overdoses in some alternative-universe Oregon that's exactly the same as the one here, except for having no new drug laws.
This approach would be perfect, methodologically speaking. The two Oregons are identical, except that in one of them, Measure 110 passes in February 2021. Any differences between the two Oregons after February 2021 would therefore be attributable to the new law. (In research lingo, the real Oregon is the experimental group, while the alternative-universe Oregon serves as a control group.)
In practice, this approach doesn't work, because researchers can't gather data from alternative universes. Perhaps that will be Elon Musk's next project. In the meantime, what Joshi and colleagues did, in effect, was to create alternative-universe Oregons and Washingtons using a statistical technique called the synthetic control method (SCM).
SCM isn't perfect either, but the underlying rationale is sensible. I'll use Oregon to illustrate. Basically, the researchers combined data from 12 other states similar to Oregon in a way that created overdose rates almost identical to what was seen for Oregon for the pre-decriminalization time period. This gives us an alternative-universe Oregon. The question then becomes: What happens in the two Oregons during the year after decriminalization occurred in the real Oregon?
Joshi and colleagues found that the overdose rates in both Oregon and Washington increased after February 2021, but increases were also observed throughout the country, including in states combined to create the alternative-universe Oregon and Washington. Decriminalization didn't have an impact one way or the other, in other words. Oregon and Washington would have experienced the same increases in overdose fatalities regardless of whether or not they implemented the new laws.
Here's the actual data:
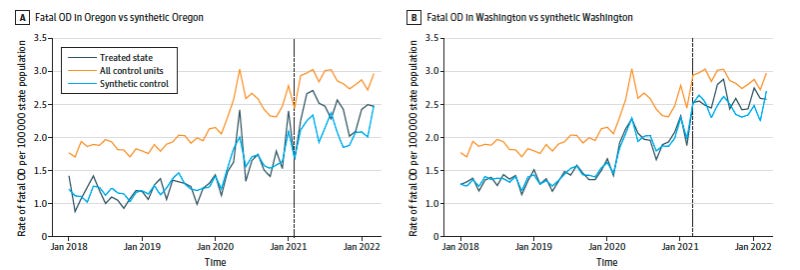
I'll continue to use Oregon as an example. In the figure on the left, the y-axis is the rate of fatal overdoses per 100,000 people, the x-axis is time, and the dotted vertical line marks the date that the new decriminalization laws took effect.
The orange line represents the average fatal overdose rates for all other states (excluding Washington) plus the district of Columbia. The dark blue line shows overdose rates for the real Oregon, while the light blue line shows the rates for the alternative-universe Oregon.
Notice that during the pre-decriminalization period, the dark blue line and the light blue line closely overlap. They do so because, as I mentioned earlier, the researchers created a single, alternative-universe Oregon from other state data that matched the real Oregon as closely as possible.
If you continue looking closely at the figure, you might eventually say: Hey, during the post-decriminalization year, the dark blue line tends to be higher than the light blue line. Doesn't that mean the real Oregon had more overdose deaths than the alternative-universe Oregon?
Yes and no. Yes, there's an absolute difference, but no, it's not a significant one. It's actually an extremely tiny difference that's magnified by the way the y-axis is scaled. Specifically, it's a difference of 0.268 deaths per 100,000 people during the year following decriminalization. That's between 2 and 3 deaths per million people.
To be clear: My point is not that the loss of two or three more lives is unimportant. Rather, because it's such a tiny, statistically non-significant difference, we can't conclude that it's genuine. There's too much room for error (e.g., in the death certificates gathered by the CDC) and for genuine variability (e.g., a slightly different pattern might've emerged if the post-decriminalization period lasted, say, 13 or 14 months. Perhaps then we might see 2 or 3 fewer deaths per million).
What do the new study findings tell us?
The new study revealed the one and only finding that doesn't clearly support either side of the decriminalization debate.
Decriminalization advocates get no support, because after February 2021, drug overdose deaths continued to increase in both Oregon and Washington. The new laws didn't alleviate the problem.
Decriminalization opponents get no support either, because after February 2021, drug overdose deaths increased in both states at about the rate they would've increased anyway, even if the laws hadn't changed. Decriminalization did not exacerbate the problem, as these opponents would've expected.
Before I say more about this, let's consider the other main source of data on Oregon and Washington.
The stories
By most accounts, drug decriminalization in Oregon and Washington has been a spectacular failure.
Narrative reports – the stories shared by local residents, investigative journalists, etc. – tell us that following decriminalization, drug use immediately became more open and undermined quality of life for all. Everyone, it seemed, had stories like the one I shared about the couple on my landing, and cities like Portland began creating, or at least trying to create, laws banning public drug use.
Stories and statistics
The stories emerging from cities like Portland and Seattle don't necessarily contradict Joshi and colleagues' findings, because they focus on different variables.
The stories tell us that following decriminalization, drug use became more open. That makes sense. Joshi and colleagues' data tell us that following decriminalization fatal overdoses didn't increase more than they would've anyway. That makes sense too.
There are different ways to draw together stories and statistics. Here's one: What makes a drug such as fentanyl more or less life-threatening is typically not the current status of drug laws in the user's state. When drug laws are lenient, users may relax a bit about where they purchase and consume the drug, but what determines whether or not they survive their next high is determined by a long list of other variables. Fatal overdoses, when they're not intentional, occur when people are careless about how much drug they take, when they mix drugs, when they're misled about the strength or contents of what they're taking, when they overdose but nobody in the vicinity has Narcan or can otherwise intervene, and so on.
What should we do?
Advocates of decriminalization say that we just need to give Oregon and Washington more time, while making sure that their prevention and treatment efforts are implemented as planned.
Opponents say that decriminalization has failed even more profoundly than the war on drugs failed, and part of any solution would be to recriminalize certain kinds of drug-related activity.
I think both sides are right, in a sense.
I have no expertise in drug policy, but I do know a bit about methodology, and it's clear that the Oregon and Washington "experiments" haven't given decriminalization of the most lethal drugs a fair test.
In Oregon, for example, state tax revenue from marijuana sales, combined with expected savings from arresting and incarcerating fewer drug users, was meant to fund treatment, but health care professionals in the state say they never had enough personnel or resources to provide adequate support. Meanwhile, people who got that $100 ticket for illicit drug use typically ignored it, or made the requisite phone call but never followed through. This April, the Economist reported that during the two-year period following decriminalization, only 40 Oregonians made that phone call and expressed interest in treatment. This tells us that Oregon's experiment isn't being carried out anywhere close to the way it was planned. If you don't run an experiment properly, you can't evaluate the data.
The best decriminalization "experiment" I've seen is being conducted in Portugal. In 2001, at the height of its own drug crisis (primarily heroin), the country decriminalized all drugs. Offenders now received penalties, such as fines, unless they attended an interview (the next day!) conducted by a psychologist or social worker, and then appeared before a commission consisting of a doctor, a lawyer, and a social worker, who would provide information about treatment and connect the person with relevant short- and long-term support. The Portuguese government provided substantial resources for prevention, treatment, and harm reduction (mobile teams, safe drug consumption facilities, etc.), and the health care system was given ample transition time.
The results of the experiment were phenomenal. By 2018, for instance, the number of heroin addicts had dropped from around 100,000 to around 25,000, and the country was spending far less money per year on managing its drug problem. Sadly, Portugal's economic difficulties, including the financial crisis of 2007-2008, led to cuts in funding for almost all drug-related programs. In 2012, these programs received more than $82.7 million U.S. dollars per year; a decade later, that figure had dropped to under $15 million. Illegal drug use and overdoses increased during the same time period. From 2019 through the present, overdose rates in Lisbon have doubled.
The message from Portugal is clear: Decriminalization of the most dangerous drugs can be surprisingly effective, but only if accompanied by sufficiently comprehensive, sustained support for offenders. Without that support, decriminalization is doomed to failure.
As for the U.S., I think the opponents of decriminalization are absolutely right: It has failed miserably in places like Oregon and Washington. But the advocates of decriminalization are right too, in the sense that we just haven't done it properly yet.
I have mixed feelings about decriminalization per se. I'm not sure whether the most effective and ethically justifiable strategy is to decrease – or increase – the strictness of current drug laws. But I do think we can separate legal practices from social ones. Whatever legal penalties states and cities impose for drug use – whether they decriminalize or recriminalize – I would like to see them devote more resources to prevention and treatment. I'll never know what drove that couple to shoot up on my landing, but even if it was merely dumb, selfish choices on their part, I think they deserve our sympathy and support.
Thanks for reading!