

Psilocybin

When I was 6 years old, I knew two things about mushrooms:
1. If you eat the poisonous kind, you'll die.
2. If you eat the magical kind, you'll see god. Then you'll die.
In fact, overdosing on "magic mushrooms" (i.e., psilocybin) is rarely fatal. My misunderstanding probably stemmed from growing up at the time when psychedelic drugs were beginning to be demonized in the U.S.
Psychedelics in the dark ages
From the 1950s through the early 1970s, psychedelics such as LSD and psilocybin were viewed as promising new tools in psychology and psychiatry. More than a thousand studies on the potential benefits of these drugs were conducted. However, in the 1960s, psychedelics escape from the lab and become street drugs, the news media sensationalizes "bad trips", Timothy Leary ("Turn on, tune in, drop out") gets fired from Harvard for unethical LSD research, and Richard Nixon is elected. In 1971, Nixon declares a "war on drugs," but by then, from a research perspective, the war was over already and science had lost. Specifically, in 1970, following the Controlled Substances Act, drugs such as LSD and psilocybin were declared Schedule I substances, meaning that they have "no currently accepted medical use and a high potential for abuse". This effectively killed research on the mental health benefits of psychedelics for three decades.
The psychedelic research renaissance
Since around 2000, when Johns Hopkins established its Center for Psychedelic & Consciousness Research, psychologically-oriented research on psychedelics has picked up again. Hundreds of studies now suggest that psychedelic drugs can aid in the treatment of psychological disorders, addictions, and the emotional challenges of terminal disease. (Public perception is shifting too, and you can even find Michael Pollan on Netflix extolling the virtues of psychedelics in his 2022 documentary "How to Change your Mind".)
A new psilocybin study
The focus of this newsletter is a study, published earlier this week, showing that psilocybin can help reduce alcohol dependence. I want to tell you about this study, because it's a great example of how caution is needed in evaluating research findings. The study has clear methodological and statistical limitations, but when you look closely, you find that these limitations aren't as bad they seem. Then, just as you conclude that the results are compelling, you discover some financial incentives behind the scenes...
Background for the study
This study, led by NYU professor Michael Bogenschutz, is the first full-blown experimental test of psilocybin's impact on alcohol dependence. In order to obtain permission for this study, the researchers had to provide an unusually thorough rationale. Here's the essence of it: (i) Existing treatments for alcohol dependence aren't very successful. (ii) Older studies suggest that just one or a few doses of other psychedelics can reduce alcohol dependence. (iii) Lower rates of alcoholism are found among groups who use psychedelics in sacred rituals. (iv) Psilocybin in particular has been shown to improve mental health and mood. (v) When administered in the lab, psilocybin is safe and can produce positive, transformative experiences that endure over time. (vi) The effects of psilocybin on the brain are consistent with changes that would reduce alcohol dependence (though the connections are mostly speculative at present).
Methods
Participants consisted of 95 adults diagnosed with alcohol dependence (according to DSM-IV criteria). The age range was 25 to 65 years. The researchers took many steps to ensure a suitable sample for this study. For example, people with known psychiatric or drug use disorders were excluded, as were people who reported use of hallucinogens in the prior year.
The study lasted for 36 weeks. All participants were provided with a total of 12 psychotherapy sessions designed to address their dependence on alcohol. (This is an important detail. The premise of the study was not that psilocybin by itself would be an effective treatment. Rather, following widespread clinical practice, it was assumed that drugs might be effective when accompanied by therapeutic support. In other words, you don't just take a pill; you also talk with a trained professional.)
At weeks 4 and 8, 49 participants received psilocybin, while the remaining 46 participants, who served as a control group, received an antihistamine called diphenhydramine. On each day of drug administration, participants remained in the lab for at least 8 hours.
The dosage of psilocybin (40 mg per 70 kg of body weight) was chosen on the basis of prior work suggesting that it could substantially alter consciousness with minimal or no side effects. For participants who weren't strongly affected by the psilocybin at week 4, dosage was increased at week 8.
In this study, participants were "blind" to condition, meaning they weren't told whether they were receiving psilocybin or the other drug. Blinding was used to rule out placebo effects – i.e., to ensure that if psilocybin turned out to be effective, the benefits would stem from its chemical composition rather than peoples' expectations about taking it. Diphenhydramine was chosen for the control condition because it does create some changes in consciousness, although it's not a hallucinogen. The researchers hoped that blinding would be successful and participants wouldn't be able to guess which drug they took.
Drinking behavior was measured by self-report. Participants were asked at weeks 8, 12, 24, and 36 to describe their drinking behavior during the prior weeks. The researchers recorded the percentage of days in which drinking occurred, the percentage of days in which heavy drinking occurred, and the average number of drinks per day. Heavy drinking was the main variable of interest.
(A "drink" was defined as any fluid containing 14 grams of alcohol. As explained to participants, that meant one 12-ounce beer, one 5-ounce glass of wine, or one shot/mixed drink. A "heavy drinking" day was a day during which a male participant had more than five drinks, or a female participant had more than four drinks.)
Results
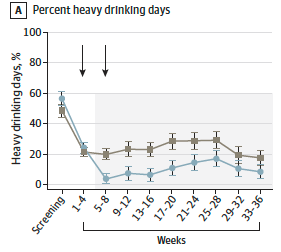
All participants sharply reduced their drinking between weeks 0 and 4, presumably due to the psychotherapy they were receiving, and to the request that they try to abstain prior to drug administration at week 4. Drinking behavior remained fairly stable after that among both groups. However, it dropped significantly more for the psilocybin group, and remained significantly lower throughout the entire 36 weeks of the study. These effects of psilocybin were seen for all three measures of drinking. For example, the figure below shows the results for percent of days in which heavy drinking occurred. The gray line represents the control group, while the light blue line represents the psilocybin group. As you can see, starting at weeks 5–8 and continuing through the end of the study, that light blue line remains below the gray one. It's not a huge difference, but it's consistent: the psilocybin group reported fewer heavy drinking days than the control group did across the remaining 7 months of the study. (Similar patterns were found for the other drinking variables.)
The researchers also tallied the number of days that participants reported being completely abstinent. Overall, the psilocybin group had roughly twice as many abstinent days as the control group. For instance, during weeks 33 through 36, the psilocybin group remained abstinent on 47.9% of the days on average, while the control group remained abstinent on 24.4% of these days. (The researchers didn't make much of this finding, perhaps because for some people, what's more important is not the number of days they abstain completely, but rather the number of days they overindulge.)
Study limitations
The results suggest that there's indeed a bit of "magic" in magic mushrooms, though not the kind we routinely think of. More studies are needed, but, in the meantime, what about these findings here? Can we trust them?
As I suggested at the outset, this study illustrates the need for caution in evaluating research findings. Experts share widely agreed-on standards for evaluation, but we shouldn't apply these standards in a simplistic, formulaic way. (I'm tempted to say that evaluating studies is an "art", but that sounds pretentious, so let's just say instead that we should allow for some nuance in the evaluation process.)
To illustrate my point, I'll describe three limitations of this study and explain why I believe each one is less serious than it seems.
1. Small sample size.
This is one of the most common limitations of experiments in which the intervention is complicated, expensive, and/or sensitive in some respect.
In this particular study, a sample size of 95 was good enough, statistically speaking, to determine whether the two groups differed in drinking behavior. (In technical terms, the main analyses were adequately powered.) Limitations only crop up when we think about using the intervention in the general population. For example, 95 participants isn't enough to compare subgroups in their response to psilocybin – e.g., to find out whether some people respond poorly to the drug – or to examine whether differences in the subjective experience of taking psilocybin influence drinking behavior. (Also, as the researchers themselves noted, it's unclear whether their results would generalize to people with more serious alcohol abuse issues.)
In my view, small sample size is partly offset here by the consistency of the results over time. For all drinking variables, at all measurement points, psilocybin outperformed the control drug. In addition, these findings are consistent with those from pilot studies on the same topic, and from studies on the use of other psychedelics to support the treatment of addiction. So, I would agree with the researchers' view that small sample size is a limitation but their results are nonetheless promising.
2. Placebo effects.
Participants were invited to guess which drug they'd received, and more than 90% of each group guessed correctly. (No surprise when you imagine the difference between how it feels to take a hallucinogenic drug versus an antihistamine.) In short, the attempt to blind participants to conditions failed, and a placebo effect can't be ruled out. Perhaps what helped people wasn't the chemical compounds in psilocybin, but rather the mere expectation that the drug would help – in which case, participants could've taken aspirin labeled as psilocybin and obtained the same benefits.
Although placebo effects undermine study findings, this is arguably less of a problem for the current study than for others. Experts in research methodology might disagree with me on this, but here's my rationale: People with alcohol dependence issues often try out new approaches to treatment with high hopes for success, only to relapse in less than a year. In other words, expectations that treatment will help don't necessarily pay off in the long run. In the present study, psilocybin continued to show benefits 7 months after administration. I see in this a hint, at least, that these benefits were not merely placebo effects.
3. Measurement error.
Participants described their own drinking behavior retrospectively. As I've discussed in other newsletters, people may incorrectly recall how much they drank. Or, they may deliberately underreport their alcohol consumption (e.g., to please the experimenter). And there's inherent messiness in asking about "drinks". Even though participants are told that a "drink" means one 12-ounce beer, or one 5-ounce glass of wine, and so forth, each brand differs in alcohol content, people don't always know the size of their glasses, they don't always finish their drinks, and individual metabolisms differ.
I'd say it's problematic, if not suspicious, that the researchers say almost nothing about the measure of drinking behavior they used. In the study itself, and in a protocol published as a separate file, they exhaustively detail every aspect of their methodology except for this one. For drinking behavior, the reader is simply assured that the measure is standard and highly reliable. To get to the details, you have to look behind a paywall (I'm fortunate to have a library privileges at my former university), and once you do, all the messiness – and limitations in reliability – are revealed.
At the same time, I'd call the prospect of measurement error a minor limitation rather than a flaw in this study, because there's no particular reason to expect the groups to be differentially affected. In other words, error is just as likely in the psilocybin group as in the control group. Of course it's possible that, by chance, the psilocybin group as a whole underestimated their alcohol consumption, but this is merely a possibility. There's no good reason to believe it actually occurred.
Conclusion and caveats
Focusing narrowly on the study itself, I find the results promising. Two doses of psilocybin slightly increased the effectiveness of psychotherapy designed to reduce alcohol dependence, and the effects persisted at least 7 months after the second dose. I just want to add two caveats that come to mind when looking around outside the study:
1. Social attitudes toward psychedelics are changing, and they may soon get ahead of the science. Since 2019, 14 cities, as well as Oregon and Washington D.C., have decriminalized psilocybin use (or de-prioritized its policing and prosecution). The Washington state legislature is now considering a bill that would decriminalize psilocybin use – California's state legislature is working on a broader bill for psychedelics – while in Colorado, voters will decide this fall whether to legalize psilocybin. At the forefront of these new trends is Berkeley professor Michael Pollan, whose 2018 bestseller "How to Change your Mind" led to the 2022 Netflix documentary of the same name. Pollan's message is that psychedelic drugs like psilocybin can be a very, very good thing, whether comforting the dying, healing the sick, or simply bettering the well.
Greater openness to psychedelics seems desirable, given evidence that they can help some people some of the time. I would love to see these drugs become a widespread option for use in psychotherapy, medical settings, and hospice care, for example. At the same time, none of the studies to date has been large enough to adequately examine subgroups – in other words, to determine who does vs. doesn't benefit from the drugs. This is especially problematic for the study I reviewed here, because the effects of psilocybin were small. In short, we're not sure whether magic mushrooms would be magical for everyone. Although I don't think science should be the last word on wellness, it's an important word, and it would be great if the experiences that Dr. Pollan and others report could be corroborated by large clinical trials.
2. At the risk of sounding cynical, here are some money-oriented observations: Michael Bogenschutz, the lead author of the study discussed here, is funded by B.More for this work. This week, the FDA granted B.More approval to proceed to the next phase of testing psilocybin as a treatment for alcohol dependence. Although B.More is a non-profit biopharmaceutical company, the company and its owners stand to reap enormous financial gains if psilocybin becomes an FDA-approved treatment for alcohol use disorder (AUD). This brings me to a press release, in which the CEO of B.More summed up the study findings as follows:
"With a reported 83% average reduction in alcohol consumption among heavy drinkers, the results of Dr. Bogenschutz's recent trial point to the clear potential of psilocybin as a breakthrough in the way we treat AUD."
The is a deeply misleading summary . As you can see from the figure I presented earlier, both the psilocybin group and the control group showed strong reductions in heavy drinking. The main dip occurred between weeks 0 and 4, and at week 4 heavy drinking was almost identical across groups – but this is before they had taken any drugs. Both groups report fewer heavy drinking days at this point, due to some combination of the psychotherapy they'd been receiving as part of the study, as well as the request that they try to stop drinking prior to drug administration at week 4.
If you want to know how effective psilocybin was, the only data that counts is the difference between groups following the administration of psilocybin or the control drug at weeks 4 and 8. From week 4 on, this difference is small but consistent (with no "boost" after week 8).
Now we can see some important context for that 83% statistic: (a) From the beginning to the end of the study, there was an 83% decline in heavy drinking for the psilocybin group, but a 51% decline was also seen for the control group – and, for both groups, most of the decline occurred prior to taking any drugs. (b) From week 4, when psilocybin was first administered, to the end of the study, the psilocybin group showed a further decline in drinking of about 10 to 15%. If you had to choose one take-away from the study, this is it. You can see it in the figure I provided. After week 4, the control group tends to stay the same or increase slightly in heavy drinking, while the psilocybin group reports a roughly 10 to 15% drop. The effects of psilocybin are small, in other words. Consistent but small.
In sum, although I can't claim to know the CEO or his motives, I do smell money lurking in the wings of his 83% remark. (There's a metaphor you might hear from someone who's currently high on psilocybin, but I can assure you that, to the best of my knowledge, I'm sober.)
Thanks for reading!